What exactly is glaucoma?
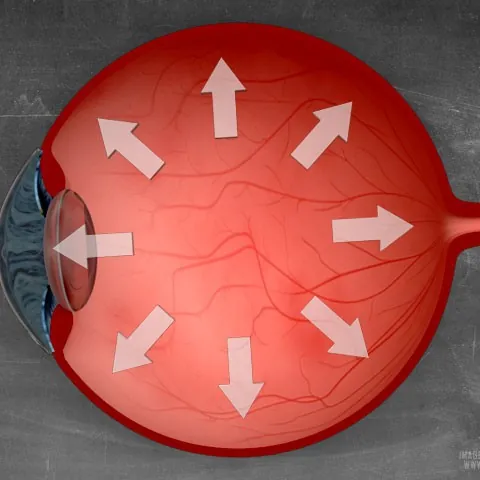
In a healthy eye, aqueous humour is continuously produced and drained through the iridocorneal angle. If drainage is hindered, intraocular pressure rises and perfusion of the optic nerve is compromised. In normal-tension glaucoma, nerve fibres die despite a normal pressure, usually due to sensitive perfusion.
Who is at risk?
- Age over 40
- Family history (glaucoma in parents or siblings)
- High myopia or hyperopia
- Diabetes, low blood pressure or sleep apnoea
- Long-term corticosteroid use
- Previous eye trauma
How do we make the diagnosis?
A single measurement is not enough. In practice we always combine several examinations:
- Intraocular pressure (tonometry): with the gold standard Goldmann applanation or a non-contact tonometer.
- Pachymetry: the corneal thickness affects the measured pressure.
- OCT of the optic nerve: measures the nerve fibre layer thickness with micrometre precision and detects loss years before any visual field defect appears.
- Visual field (perimetry): maps any blind spots.
- Gonioscopy: assessment of the iridocorneal angle (open or closed).
Treatment
Glaucoma cannot be cured but can be kept perfectly under control by lowering intraocular pressure. The choice depends on the type and severity:
- Pressure-lowering drops: first choice. Often one drop per day (prostaglandin analogues).
- SLT (Selective Laser Trabeculoplasty): a short laser treatment in the iridocorneal angle; lowers pressure for 3-5 years and can be repeated.
- MIGS (Minimally Invasive Glaucoma Surgery): micro-implants that improve outflow of aqueous humour.
- Filtration surgery (trabeculectomy, tube shunt): for advanced cases.
How often should I be checked?
From age 45 a two-yearly screening is recommended; from 60 yearly. With a family history we start earlier. Once the diagnosis is made, patients are followed every 4-6 months. When screening is combined with a cataract operation, a MIGS implant in the same procedure can further reduce intraocular pressure.
Related topics
- Diabetic retinopathy — retinal damage from diabetes, requires yearly follow-up.
- Overview of all eye treatments
- About Dr Isabel Pinxten — your treating ophthalmologist, FEBO and head of ophthalmology at AZ Zeno.
- Practical consultation info or directly book an appointment.