How does retinopathy develop?
Long-term elevated blood sugar damages the wall of retinal capillaries. Micro-aneurysms, bleeds and exudates appear (non-proliferative retinopathy). At an advanced stage, the retina forms new, fragile vessels (proliferative retinopathy) which can bleed into the vitreous or cause macular oedema.
Macular oedema
Fluid can also leak into the central retina (the macula): diabetic macular oedema. This is the most common cause of vision loss in diabetes and can already occur in the early stages.
Which examinations do we perform?
- Dilated fundus exam: pupil dilation for a complete view of the retina.
- Colour fundus photo (retinography): reference document for follow-up.
- Macular OCT: measures any oedema with micrometre precision.
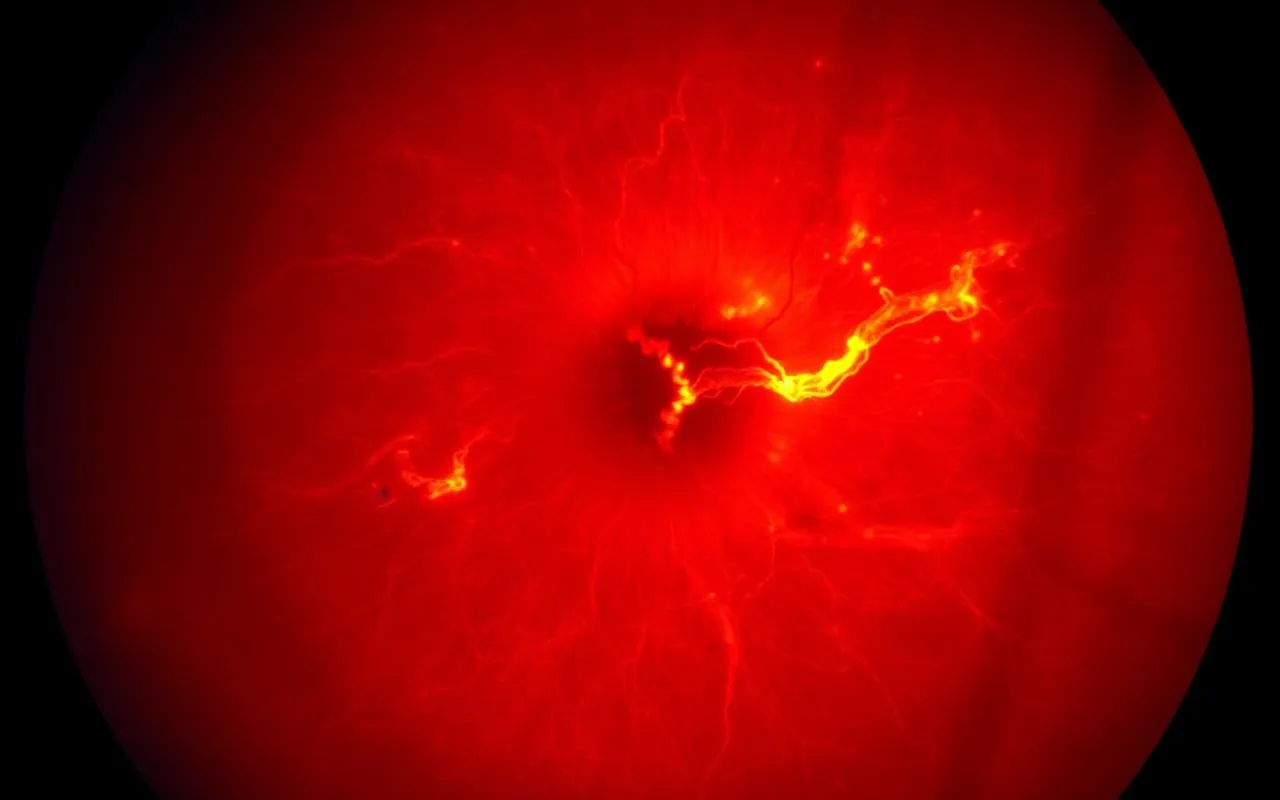
- OCT angiography or fluorescein angiography: visualises retinal perfusion in advanced stages.
Treatment options
- Glycaemic, blood pressure and cholesterol control: the most important baseline treatment, in collaboration with your endocrinologist and GP.
- Intravitreal injections (anti-VEGF): for macular oedema or proliferative forms. A fine injection into the vitreous, ambulatory and painless under drop anaesthesia.
- Panretinal photocoagulation (laser): for advanced proliferative retinopathy, to stop neovascularisation.
- Vitrectomy: surgical removal of bleeds or tractional membranes, in close collaboration with a vitreoretinal surgeon.
How often should I be checked?
- Type 1 diabetes: yearly, from 5 years after diagnosis.
- Type 2 diabetes: yearly, from diagnosis.
- Pregnancy in diabetes: at the start of pregnancy and every trimester.
Related topics
- Glaucoma — diabetes also increases the risk of glaucoma; screening is combined whenever possible.
- Cataract — diabetic patients often develop cataract at a younger age.
- Overview of all eye treatments
- About Dr Isabel Pinxten — FEBO ophthalmologist, experienced in retinal pathology and intravitreal injections.
- Practical consultation info or directly book an appointment.